
Are the tradeoffs of prior authorization value it?
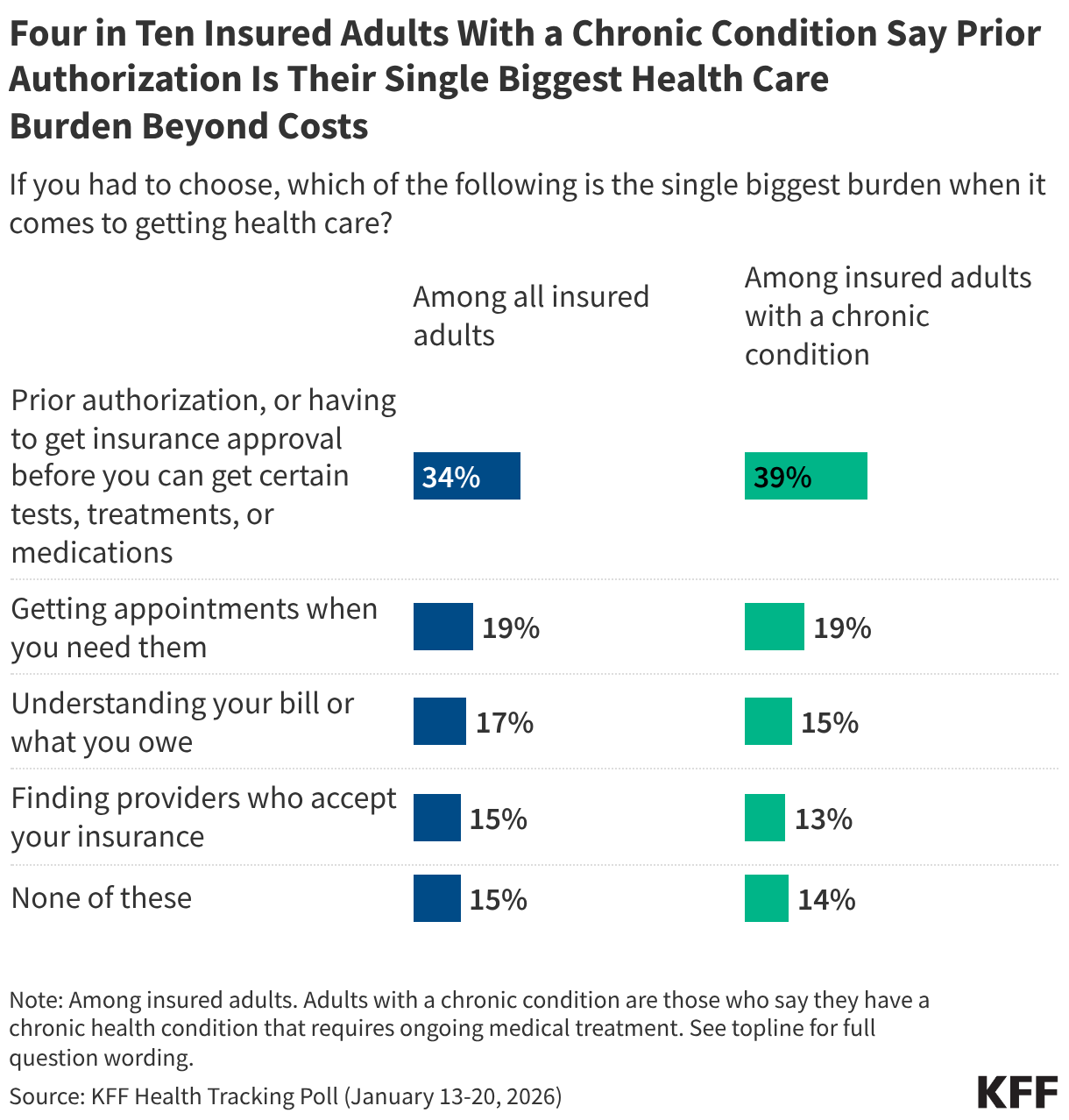
Price is the well being care problem of most concern to the American individuals. However nothing makes American healthcare customers extra annoyed when utilizing the healthcare system than a previous authorization evaluation. I do know as a result of they informed us so, placing prior authorization evaluation far forward of every other points they’ve in getting care and navigating the well being care system, together with getting appointments and understanding their payments. 4 in 10 individuals with continual situations say getting well being care is their greatest burden.
Take Medicare Benefit plans for example. In 2024, they carried out 53 million prior authorization evaluations, practically two per enrollee, and rejected 7%. what it takes to get approval. Typically quite a few cellphone calls and messages in apps to your insurance coverage firm and physician’s workplace, which in some instances culminates in a “peer-to-peer” evaluation between the physician and the insurance coverage firm (are they “peer-to-peer” on this relationship?). Stress. Delay. Generally hours on the cellphone or days ready for a name again. And generally the result’s an approval solely to find that the situation is denied or out of community, or that the quantity of drug the affected person has been taking for years requires a separate annual pre-approval. The issue is just not restricted to Medicare Benefit, it exists throughout your complete insurance coverage system besides conventional Medicare (extra on that beneath).
Healthcare professionals additionally do not like prior authorization, particularly specialists who order costlier checks and procedures and must run the gauntlet of the prior authorization course of to get them permitted. Their administrative workers fights with the insurance coverage firm workers every day. More and more, AIs from suppliers and AIs from insurance coverage firms are attempting to outsmart one another in assessments. Everybody thinks they’re sacrosanct on this tug-of-war: the physicians who see the insurance coverage firms as grasping profiteers who violate their skilled judgment, and the insurers who see themselves as the road of protection in opposition to physicians who typically don’t adhere to greatest apply tips or have a monetary curiosity in doing extra in a fee-for-service system.
There may be some disagreement about whether or not prior authorization evaluation reduces prices to payers and protects high quality by denying pointless companies or shifting care to equally efficient, cheaper companies, or whether or not it will increase prices and results in adversarial outcomes over time by delaying or denying wanted care, and there are research out there to help each claims. This isn’t the place for a literature evaluation, besides that prior authorization can and does do each. Nonetheless, there ought to be no debate that this will increase the complexity of our healthcare system, frustrates sufferers and healthcare suppliers, and drives up administrative prices.
The idea has been that we’re caught with this. Payers have few instruments in our system to manage prices, and prior authorization is one among them. However now that there’s such deep public worry about it, it is time to ask whether or not it is definitely worth the trade-off.
Present efforts to vary the evaluation of prior authorization are centered on incremental reforms geared toward making it much less burdensome. States have launched a sequence of reforms to streamline prior authorization evaluations, exempt docs with good monitor information from evaluation, droop prior authorization for persevering with take care of some individuals with continual situations, require docs to double-check evaluations of insurance coverage firm AIs, and extra. The Trump administration has additionally joined the struggle, saying a voluntary effort with main well being insurers to hurry up and simplify prior authorization evaluations, together with reforms that promise to chop again on what’s reviewed and the way typically. We have to begin seeing how actual this voluntary effort is that this yr.
The larger query, nonetheless, is: can we abolish prior consent fully? I can not consider something that will be extra politically standard for a candidate planning a mid-term or 2028 platform on well being care, though a debate over whether or not premiums would rise, fueled by insurers, would possibly dampen enthusiasm considerably.
One method I used to debate with my buddy, the late Uwe Reinhardt, the good well being economist and frequent critic of insurance coverage firms, was to take prior authorization evaluation out of the palms of insurance coverage firms altogether and create impartial, physician-led nonprofits to take over the duty. That may take away the inducement that insurance coverage firms have within the present system to place income earlier than sufferers. Nonetheless, it trades a big and already established company paperwork for a completely new nonprofit that must be constructed and funded throughout the nation (I assume it might be largely funded by a tenth of well being plans, very like ACA Marketplaces do).
As well being coverage historians amongst us will know, we tried one thing like this years in the past and whereas it did not work like prior authorization immediately, the expertise was instructional. It was referred to as the Skilled Requirements Evaluate Group (PSRO) program and was administered by CMS (then HCFA) by the Well being Requirements and High quality Bureau. PSROs—physician-run nonprofits throughout the nation, funded by Congress—tried to manage prices by reviewing hospitalizations and hospital stays, with a detrimental determination ensuing within the denial of reimbursement by Medicare or Medicaid. In the end, this system was deemed to price greater than it generated and was withdrawn in 1982, when the main target usually shifted from price to high quality in a extra anti-regulatory setting.
One other method could be to comply with conventional Medicare, which has no prior authorization examine besides in very restricted circumstances. Insurers will likely be fast to say that premiums will rise even additional with out prior authorization checks. They might be proper, despite the fact that it additionally drives up prices to the well being care system in the long term by delaying and denying some needed care and growing administrative prices. A research by Milliman, which I mentioned in an earlier column, calculated the ranges for potential premium will increase. It’s also potential that prior authorization has a chilling impact on docs and hospitals simply by being there, which nobody has calculated.
However it isn’t trivial that conventional Medicare has operated nearly totally with out prior authorization evaluation. Solely not too long ago, the Trump administration—some would intuitively say that prior authorization is now so unpopular—determined to experiment with introducing it by an illustration undertaking referred to as WISeR, the Wasteful and Inappropriate Service Discount Mannequin, to check prior authorization for choose companies in six states. WISeR evaluations are, maybe surprisingly given the general public’s mistrust, pushed primarily by AI, which is seen as a advantage by its proponents.
Medicare was in a position to get by with out prior authorization, largely by paying suppliers considerably lower than personal insurance coverage pays them, fairly than by reviewing each process, take a look at or prescription to manage prices. It suggests a Medicare-like method as one possibility: eliminating prior authorization checks in trade for a discount in funds to well being care suppliers (e.g., 2%, for illustration). In actual fact, it will be a discount, buying and selling modestly decrease funds for better skilled autonomy and decrease administrative prices for physicians. It might be piloted on a voluntary foundation by a big, self-insured employer, by a public program, or throughout the system. I am unsure if suppliers would welcome the deal or not. The burden of prior authorization evaluation doesn’t fall equally on all practices and suppliers. I do know that, relying on the kind of physicians surveyed, between a 3rd and a half of physicians say they might not wish to apply drugs in the event that they needed to do it once more, largely due to the perceived lack of skilled autonomy. Hospitals would primarily profit from decrease administrative prices and will have much less curiosity. The concept wouldn’t be simple to implement.
Any transfer away from fee-for-service cost may additionally cut back the necessity for prior consent evaluation by lowering the inducement to supply extra companies. In built-in techniques similar to Kaiser Permanente (no connection to KFF), physicians with a wage haven’t any monetary incentive to supply extra care and the medical group to which they belong makes the judgment about evidence-based care.
Each change in healthcare coverage comes with tradeoffs. There are at present solely a restricted variety of instruments payers must cowl healthcare prices, and prior authorization is one among them. However in a healthcare system tormented by each complexity and excessive prices, it’s now public enemy primary for healthcare customers, particularly customers who change into sufferers and require excessive ranges of care. The intense query we’re not asking is whether or not the short-term price containment advantages for insurers and their purchasers are value the price to sufferers and healthcare professionals in an already labyrinthine healthcare system?
So the massive query: Given all of the issues, would you eliminate the prior authorization evaluation, or would you persist with the trail we’re on now and attempt to make it slightly bit higher incrementally?
See all of Drew’s Past the Knowledge columns